
Lipfendra Brings PCSK9i Efficacy with Oral Convenience
Last week, Merck’s PCSK9 inhibitor, Lipfendra (enlicitide), was approved (1) for lowering LDL-C as an adjunct to diet and exercise in adults with hypercholesterolemia. PCSK9 inhibitors are powerful drugs that offer an add-on or monotherapy option for patients who have not reached their LDL-C goals on statins alone or who cannot tolerate statins.
Trials of other drugs, including Repatha (evolocumab, Amgen), have demonstrated that lowering LDL-C with statins or PCSK9 inhibitors can lower risk of major adverse cardiovascular events (MACE) in adults at increased risk for MACE (primary prevention) or who have already had a MACE (secondary prevention).
Lipfendra’s effect on cardiovascular outcomes is still being evaluated in the CORALreef Outcomes trial (2). Using existing data and reasonable assumptions about what future outcomes data may look like, the Equinox model can estimate how Lipfendra may measure up in primary and secondary prevention.
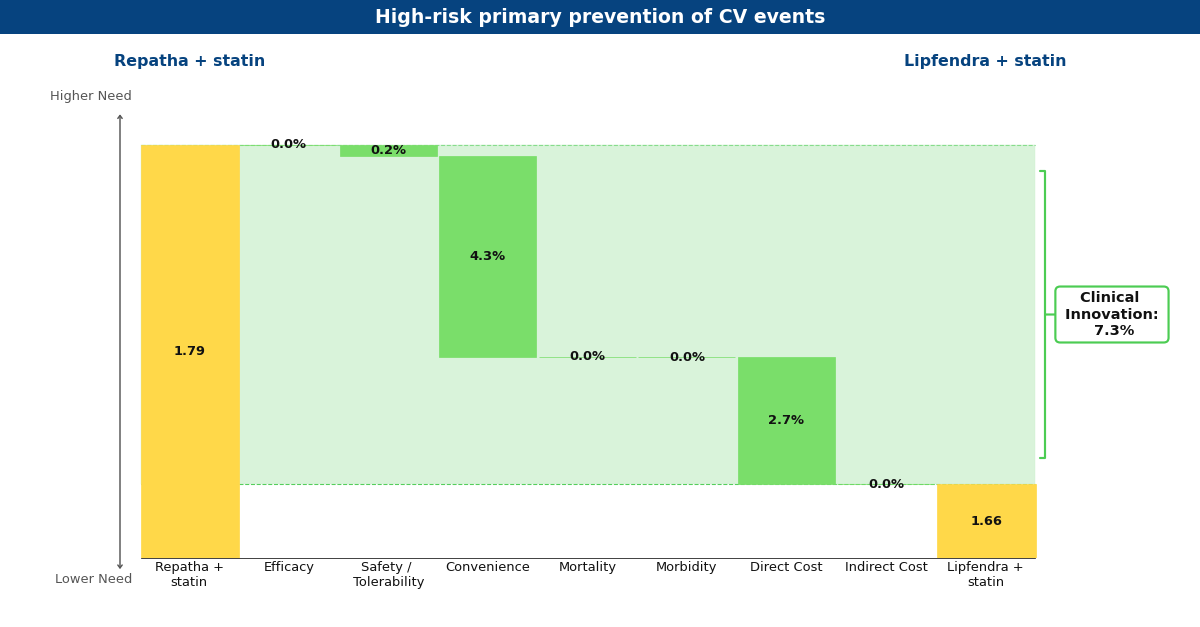
Drivers chart depicting what Equinox believes Lipfendra may look like in the future compared to Repatha for primary prevention of MACE in high-risk patients.
Lipfendra’s main driver of improvement is convenience, as it is the first approved oral PCSK9 inhibitor in a market of injectables. In Repatha’s Phase 3 MACE prevention trials (3, 4) and Lipfendra’s Phase 3 hypercholesterolemia trial (5), these drugs appeared to have a similar net-of-placebo effect on LDL-C reduction and both were well-tolerated. Based on these data, Equinox believes if Lipfendra were to be approved for primary and secondary prevention, it would be based on data demonstrating a similar tolerability and relative risk reduction in MACE as seen with Repatha.
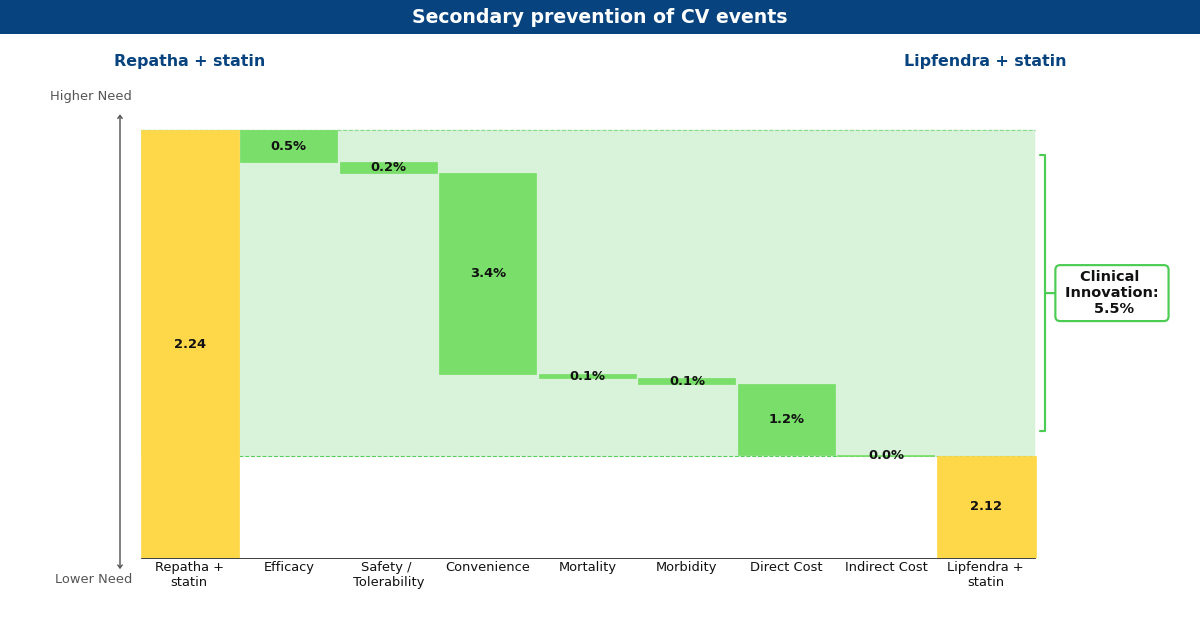
Drivers chart depicting what Equinox believes Lipfendra may look like in the future compared to Repatha for secondary prevention of MACE
Currently, Lipfendra has a substantially lower annual WAC than Repatha, resulting in overall innovation scores of 7.3% and 5.5% in primary and secondary prevention, respectively. We expect that the arrival of biosimilar Repatha will degrade this advantage somewhat, but Lipfendra would remain differentiated and commercially successful in both populations (at 6.1% and 5.0%).
Keytruda Grabs its 42nd Approval in PD-L1+ PROC
Keytruda (pembrolizumab, Merck) received its 42nd approval from the FDA this Tuesday, February 10th based on the results from the phase 3 KEYNOTE-B96 trial, which looked at the blockbuster PD-1 inhibitor as an add-on to paclitaxel with or without bevacizumab in PD-L1+ platinum-resistant ovarian cancer (PROC). [1] This subset of ovarian cancer patients has developed resistance to standard platinum-based regimens. As a result, they receive non-platinum chemotherapy, such as paclitaxel, pegylated liposomal doxorubicin, or topotecan.
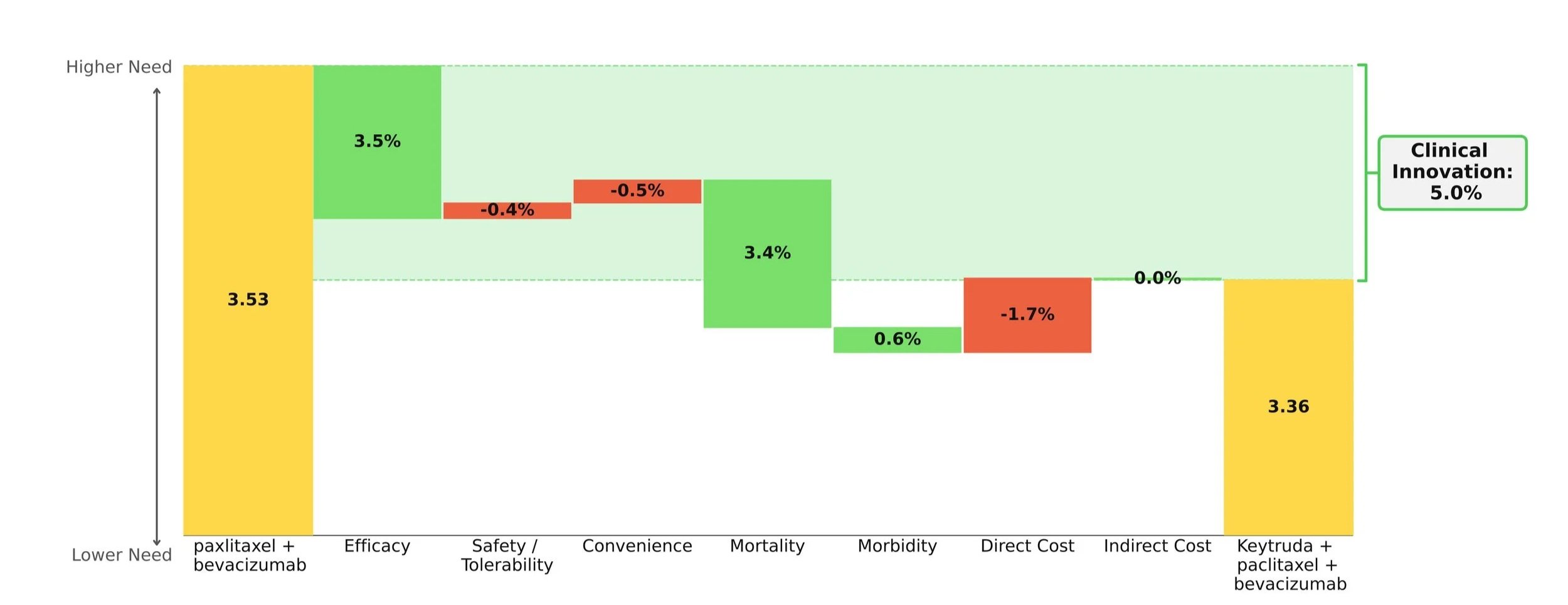
When compared to paclitaxel +/- bevacizumab, the Keytruda regimen showed improvements in survival, progression, and response while maintaining a comparable safety and convenience profile. Importantly, the mortality benefit is what stole the show: an impressive 30% increase in mOS over paclitaxel +/- bevacizumab (19.2 months vs. 14.0 months). [2]
Taking into account the cost impact of adding on Keytruda, the Clinical Innovation is clawed back slightly to a respectable 5.0% overall (Figure 1). Although Keytruda has seen higher levels of innovation elsewhere, such as its many NSCLC indications, a score of 5% typically suggests market differentiation and shows promise for Keytruda's use in this space.
This Clinical Innovation exhibited by Keytruda will increase in the coming years, as Keytruda is scheduled to lose exclusivity in 2028, which will slightly ease the cost burden.
[1] U.S. Food and Drug Administration. FDA approves pembrolizumab with paclitaxel for platinum-resistant epithelial ovarian, fallopian tube, or primary peritoneal carcinoma. February 10, 2026. Accessed February 12, 2026.
[2] Cortese T. Pembrolizumab combo significantly improves PFS/OS in recurrent PROC. CancerNetwork. October 18, 2025. Accessed February 12, 2026.
Weighing Efficacy vs. Tolerability: Lenvima + Keytruda in Advanced ccRCC
Conclusion: Despite its toxicity, the overwhelming efficacy advantage of the Keytruda + Lenvima regimen in first-line (1L) treatment of advanced clear cell renal cell carcinoma (ccRCC) puts it in a position to lead the market in this indication. Tolerability concerns will limit its share.
Winning an FDA approval in August 2021, the combination of Lenvima (lenvatinib, Merck + Eisai) and Keytruda (pembrolizumab, Merck) is the most recently approved TKI/IO therapy with an NCCN category 1 recommendation for 1L treatment of advanced ccRCC. This is the third TKI/IO combination to secure an FDA approval and category 1 recommendation, with Inlyta (axitinib, Pfizer) + Keytruda being approved in April 2019, and Cabometyx (cabozantinib, Exelixis) + Opdivo (nivolumab, BMS) approved in January 2021. The approvals and category 1 recommendations of these regimens span all risk groups. These regimens have since bumped sunitinib (Sutent by Pfizer, which went generic in August 2021) from a category 1 recommendation to a category 2A recommendation. Our comparison of the category 1 TKI/IO regimens in this indication shows that although the Lenvima + Keytruda regimen may be more toxic than the others, this disadvantage is modest relative to its major improvement in efficacy. Our analysis is based on phase 3 clinical trial data (CLEAR, CheckMate 9ER, and KEYNOTE-426).

Historically, new regimens with clinical innovation over 10% achieve strong patient share. Lenvima + Keytruda shows 13.4% clinical innovation over Inlyta + Keytruda, driven by improved efficacy.
Lenvima + Keytruda should excel commercially in patients who are able to tolerate it. Dose reductions and interruptions will help manage the toxicity of this regimen and expand its usage to patients who may not able to tolerate it otherwise.

For the clinical benefit that Lenvima + Keytruda provides relative to Inlyta + Keytruda, its higher price is reasonable. Because of this, it falls within the “cloud” of drugs that have historically achieved good market access, and we predict that Lenvima + Keytruda will perform well commercially.

As a side note, Cabometyx + Opdivo is likely to capture share in this indication as a more tolerable alternative to Lenvima + Keytruda, with its efficacy improvement driving its 7.1% clinical innovation over Inlyta + Keytruda.